

How I Used a Conjugate Strategy and the Bulgarian Method for an Acute Post-Surgical Case
Clinical case study: Reestablishing the Neurological Network of Hip Joint Function in a Clinical Setting

On May 9, I had a client come in who, two days prior, underwent bilateral hip joint surgery to repair cam impingements on both hips and both labrums. He was dropped off at my home office by a family member and accompanied by a hospital-issued walker.
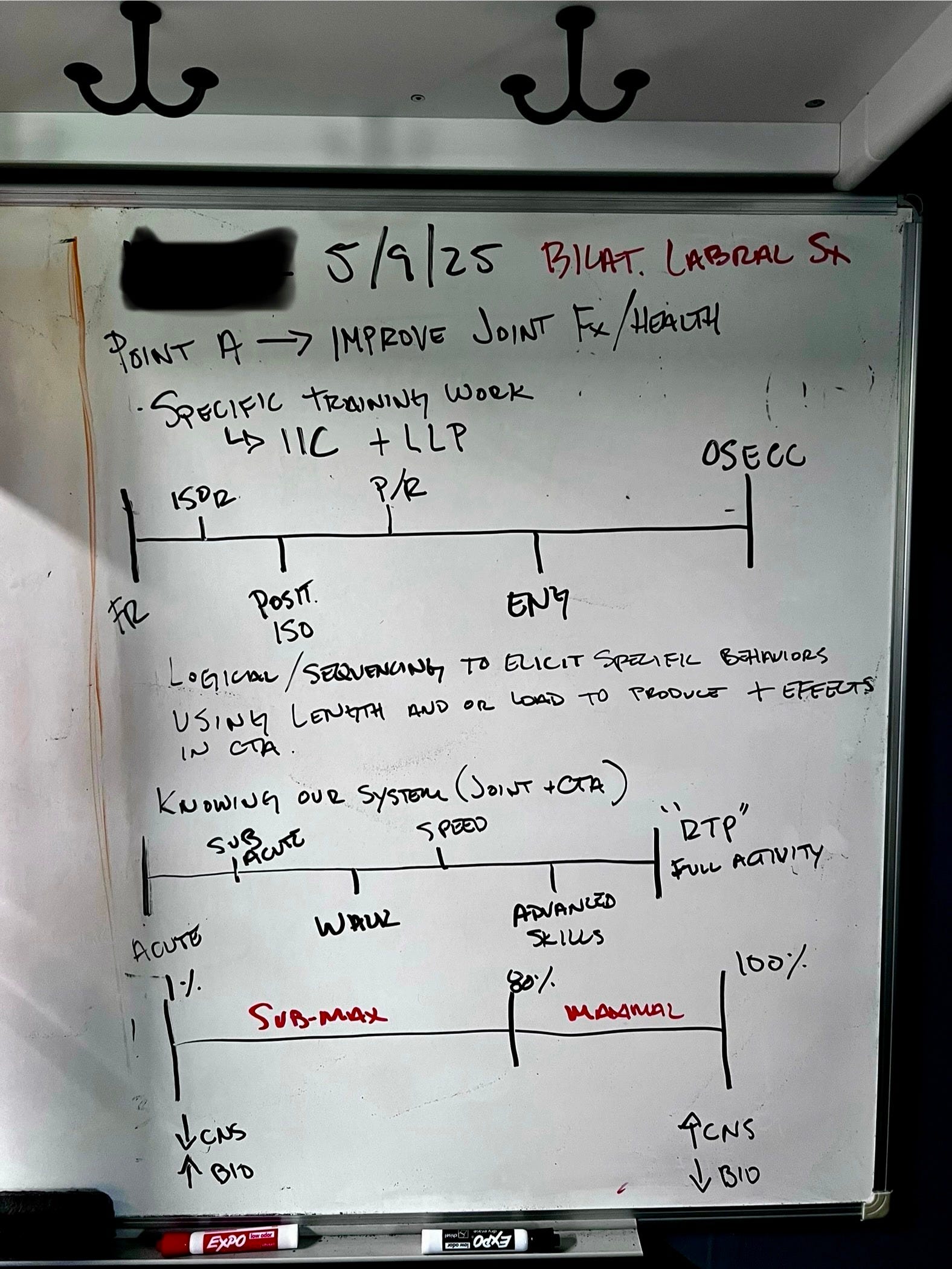
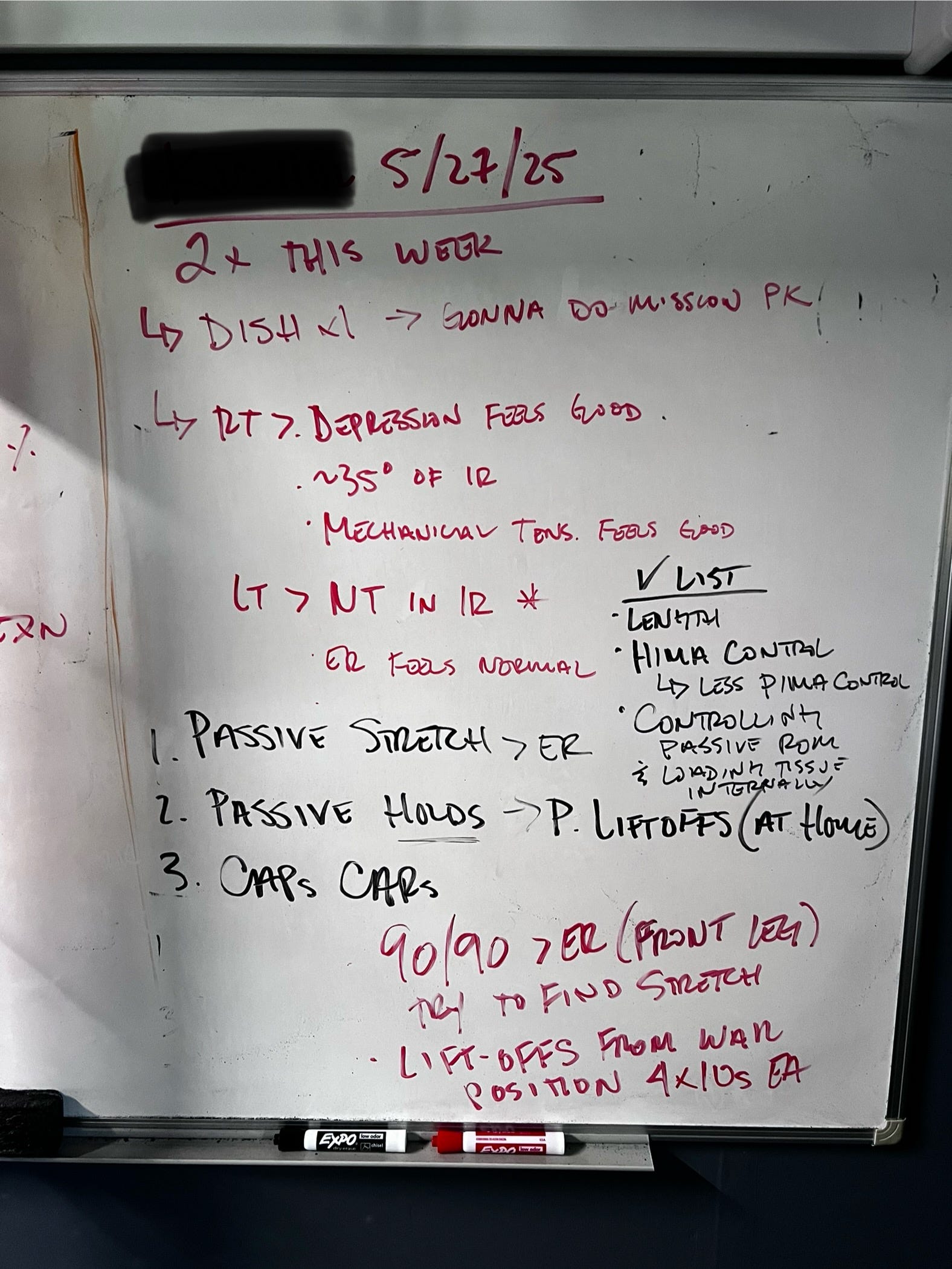
I had my whiteboard prepared with notes for our discussion. Written on the board was the length-loading progression and the internal isometric continuum.
I have worked with this individual in the past, but this time he’s a whole other case that needs a whole other strategy of care.
Point A
In our discussion, he explained how he was experiencing no symptoms whatsoever after surgery. No pain, sleeping ok, or any other major concerns. He also told me his plans to go to Switzerland in early June, where he will be hiking and visiting friends. This left us with only five clinical sessions and his at-home training in between sessions to improve his joint function to a point where his hips won’t be a problem traveling, hiking, and being a tourist.
FRA & Findings 5/9
Given what we already know about the joint, having just had surgery 48 hours prior, I felt it wasn’t prudent to assess passive ranges of motion of the hips, given I likely wouldn’t find mechanical tension.
Instead, we assessed the active capsular workspace to gauge where he was comfortable working. I also provided him with some assistance in keeping his thigh in position while he rotated his hip for peace of mind.
Once we established his ranges, I referred him back to the whiteboard and to our loading strategies. We weren’t going to do Functional Range Release and manual work, and we weren’t going to be working at length. Rather, we were going to load the “stuff” in the area and start to shine a light on that joint to reestablish the neurological net and begin reconnecting nodes.
Using HIMAs
The use of holding isometrics, or HIMAs, was my strategy for multiple reasons. One reason is that I assumed his nervous system could push harder and output a greater force than his connective tissue can withstand. Second, the HIMAs were our means to do isometric ramping on a bit larger scale. Rather than focusing on one spot on a tissue, I just wanted him to contract and control deep hip tissue. Whereby, I would simultaneously cue him to “hold and don’t let me move you”, with a tactile cue of “from this stuff right here”.
This strategy allows us to gently load the tissues and architecture not at length, and also allows the nervous system to learn, or relearn, about controlling specific musculature of the deep hip. This dual-ecology method is conjugate training and slowly reconnecting the nodes of the neurological network (sensory layer and hidden layer) of joint function, a component of Point B.
Week 1: At-home Training
We used the Bulgarian Method to train these ecologies at home, and trained twice per day.
We used a 1:1 ratio of isometric ramping in conjunction with capsular articulations every minute on the minute for 5 minutes twice daily. We do a 10-second isometric ramp followed by a zone capsular CARs (internal or external rotation) or a full capsule articulation (IR + ER) and rest the remainder of the minute.
10-second Isometric Ramp
Capsule CARs x1
Rest
Repeat at the top of the minute for 5 minutes
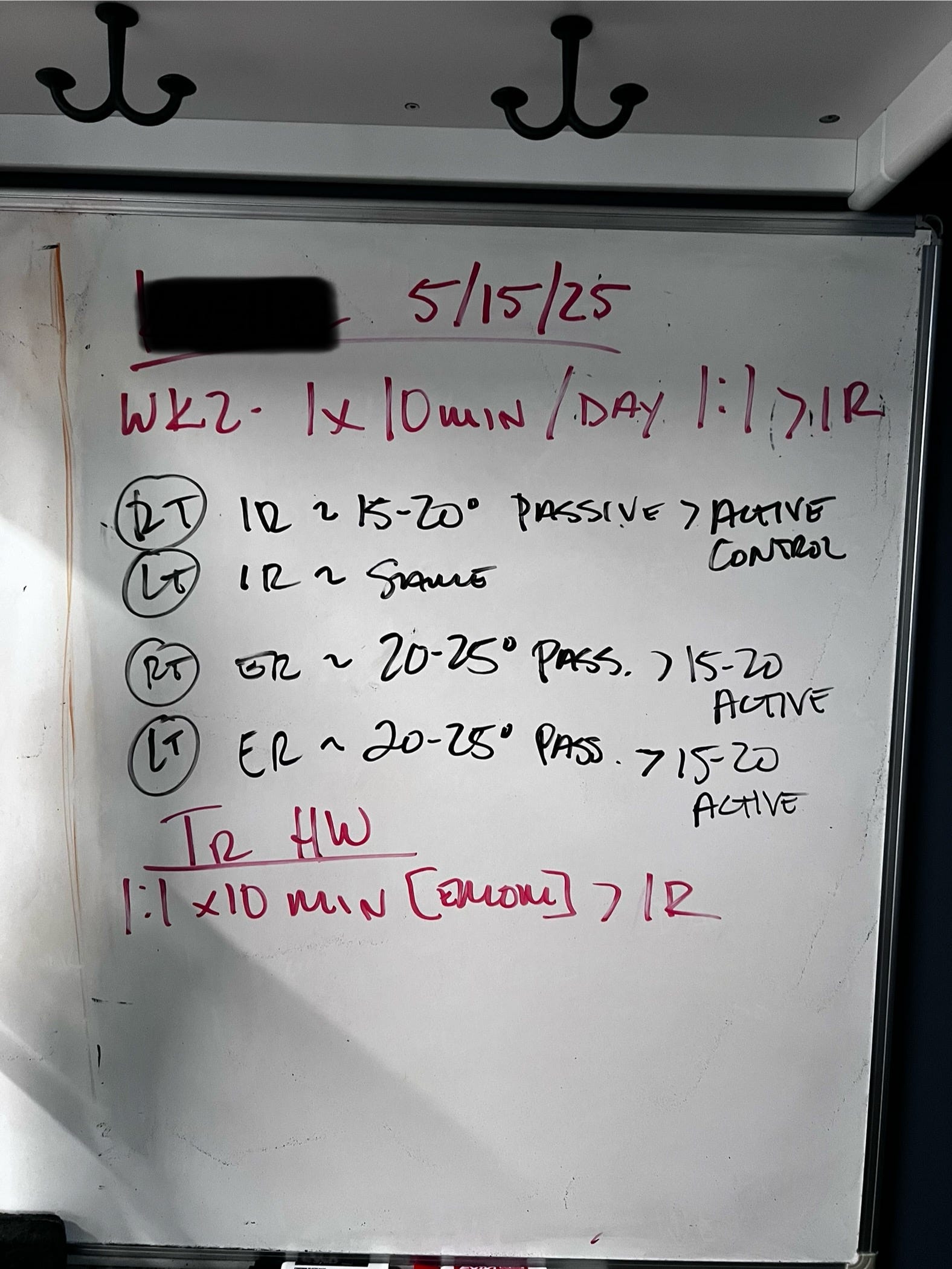
Week 2: 5/15
Feedback: The client was still asymptomatic and was experiencing zero pain. He had foregone the walker and was already taking lengthy daily walks and adhering to his twice-daily training routine.
FRA
This week, I performed passive and active table tests for rotations of the hip joint, in both internal and external rotation. I needed to feel how his hips behave. After all, if he was walking as much as he had and experiencing no symptoms, I figured he could tolerate a passive range of motion assessment.
Erring on the side of caution, though, I only moved his hips into where I felt the initial sensation of mechanical tension and a smidgen more. Followed by his active range of motion, which he felt comfortable pushing into.
He did have decent active control of his hips in both internal and external rotation, being within the 15-20 degrees of passive that we like to see as manual practitioners.
Given our findings, we continued using HIMAs and capsular articulations (CARs) as our training stimulus. Focusing on internal rotation and bumping up his total training volume to two 5-minute training bouts.
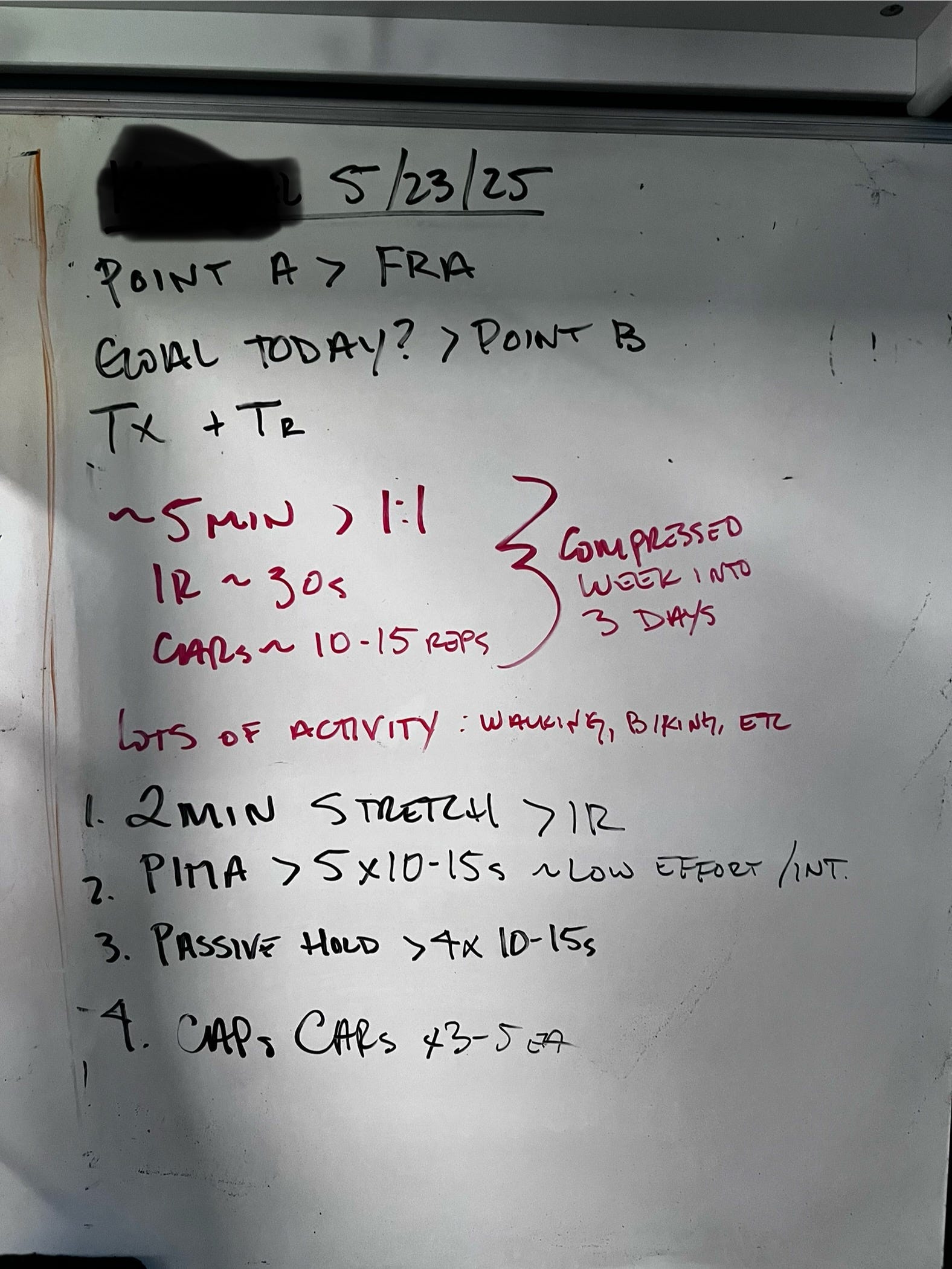
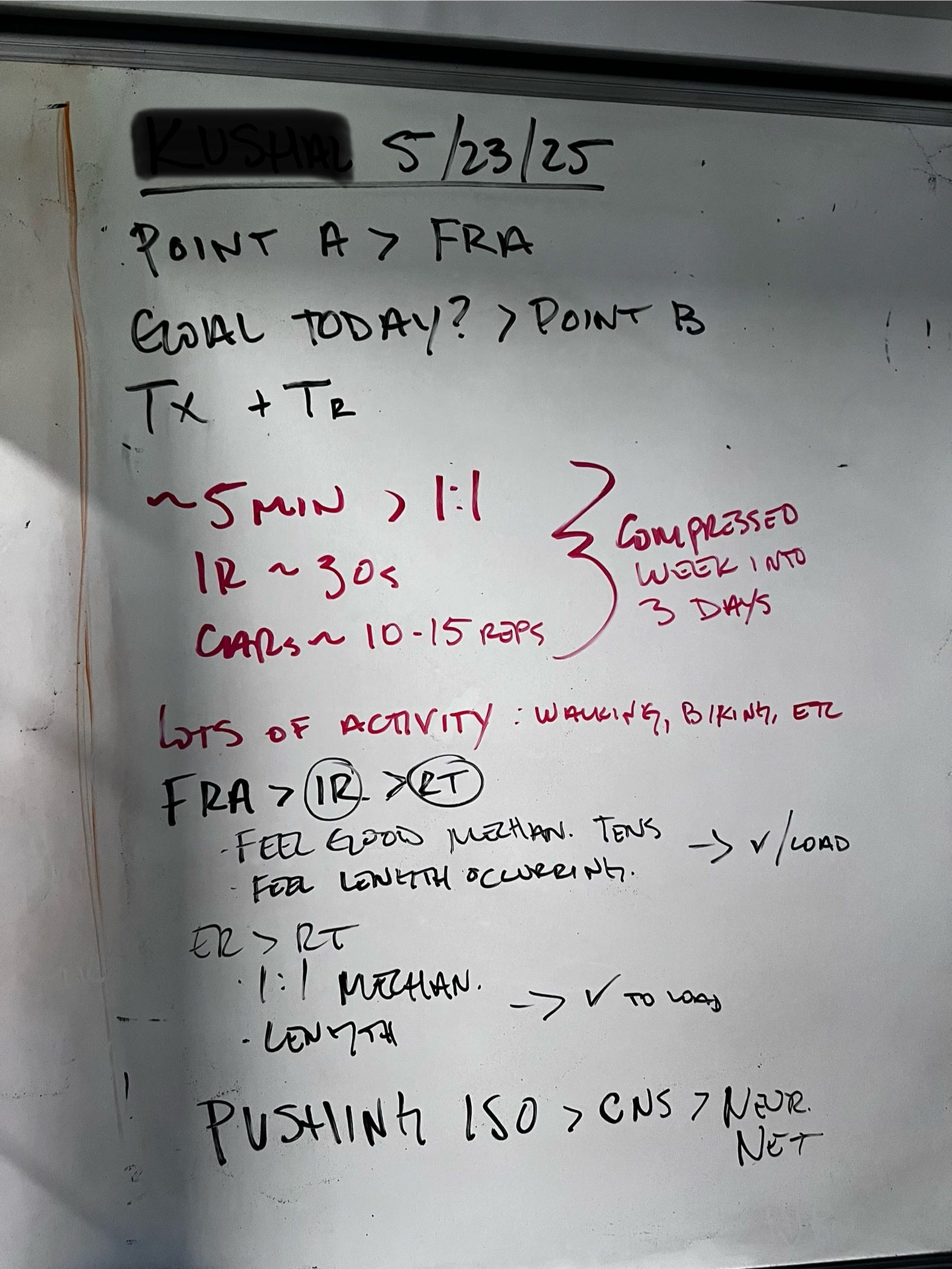
Week 3: FRA and Treatment: 5/23
He has again increased his low-level activities to long walks and using the recumbent bike. Still experiencing zero side effects of any kind from surgery. His quality of sleep also improved.
During our table tests, I too bumped it up. Actually feeling and exploring the mechanical tension of the joint capsule and tissues, which led us to find a stretch. An indicator that the connective tissue architecture is able to lengthen and transmit a signal to the nervous system. Stimulating the sensory layer of the neurological network. It was nice for us both to experience this in both internal and external rotation on both hip joints as well.
These findings allowed us to add another input and change our isometric loading strategy. We could now train the architecture at length rather than positionally.
This also meant we were able to incorporate the nervous system more so by doing pushing isometrics, or PIMAs, and thus connecting more nodes of the neural net.
Training Homework: 2x daily
2-minute stretch for internal rotation (feet on wall)
PIMA 5x10sec at a low intensity/effort
Passive hold 4x10sec
Capsule CARs (IR + ER) 1x5 each direction
Week 4: FRA 5/27
This was our final week together, and we had two sessions booked to assess and make one last push.
In my passive assessment, I was able to load his hips more with a posterior glide, which was huge. We had expanded his passive range of motion and gained more active control of both internal and external rotation in both hips.
For our manual treatment, we switched the capsule work to focus more on external rotation at this point as well.
We attempted three different training positions for him to do on his own and landed on the sundial position with a yoga block to replicate the posterior glide.
Training Homework: 2x daily
External rotation stretch 1x2min
Liftoffs/Holds 4x10sec
Zone Capsule CARs for external rotation
5/29: Save the Best for Last
This was our final visit for a while. This is where we wanted to check indicators and gain feedback; that he’d be as ready as could be in our few weeks of treatment and training for his Switzerland trip.
Side note: For added context, the day prior, he had a visit with a physical therapist to do a “capacity test.” These tests were things like a dumbbell goblet squat with the heels elevated on a slant board for sets of 15 reps. Followed by sets of 15 reps of leg curls using a physio ball. The therapist wanted to observe if his quads and hamstrings could handle the workload of his hike.
In my opinion, these tests were irrelevant given their nature. Two reasons: one is that he's going to take more than 45 steps on his hike (3 sets of 15 reps). Secondly, these are muscle “threshold” tests and observations. They did not provide any information as to whether or not his recently operated-on hips had the capacities to withstand a lengthy hike in Switzerland.
FRA and Indicators
My job as a manual therapist is to test and observe the levels of adaptation, to ensure that the athlete can “survive” at the level of competition. In this case, his level of competition is his hike.
Our focus over the past few weeks has explicitly been sequenced to ensure positive training effects in the in the passive and active joint and capsular workspaces, create healthy connective tissue architecture that can lengthen and transmit forces and other information, and be able to load said architecture by consciously controlling and contracting and by driving/pushing force into it (PIMAs and HIMAs). Lastly, being able to actively control the outermost capsular ranges of motion (Capsular CARs).
These observations will objectively give us feedback that he and his hips are indeed in a good place for his competition/hike, whilst simultaneously giving him the confidence to enjoy his experience without having to worry about hurting himself.
In our assessment, we had great improvement in his passive rotational movements; we were able to feel and experience length and normal mechanical tension, he was able to push isometrically with ease and from the appropriate “stuff”, he was able to actively hold his passive ranges of motion and resist, and he was able to actively control much of his passive ranges of motion with his capsular CARs.
Since this final session, he has successfully completed one practice hike, which, the most common trail is 6 miles round trip, and over 2,000 feet of elevation. I also suggested a couple of strategies to offer more peace of mind on his hikes. I told him to use walking sticks, or at least bring a pair just in case, and to zig-zag or tack his way on the descent to mitigate any unnecessary pounding on the knees and hips.
In Conclusion
All in all, our conjugate strategy using the Bulgarian Method to treat and train multiple ecologies and capacities to improve joint health and function to ultimately strengthen the connectedness of the neural net proved to be superior and successful in getting him from Point A to Point B.
Credit
Absolute: The Art and Science of Human Performance
Establishing Point A
Establishing Point B
Louie Simmons. Bulgarian Method and Conjugate Strategy
Love these case studies Brian.